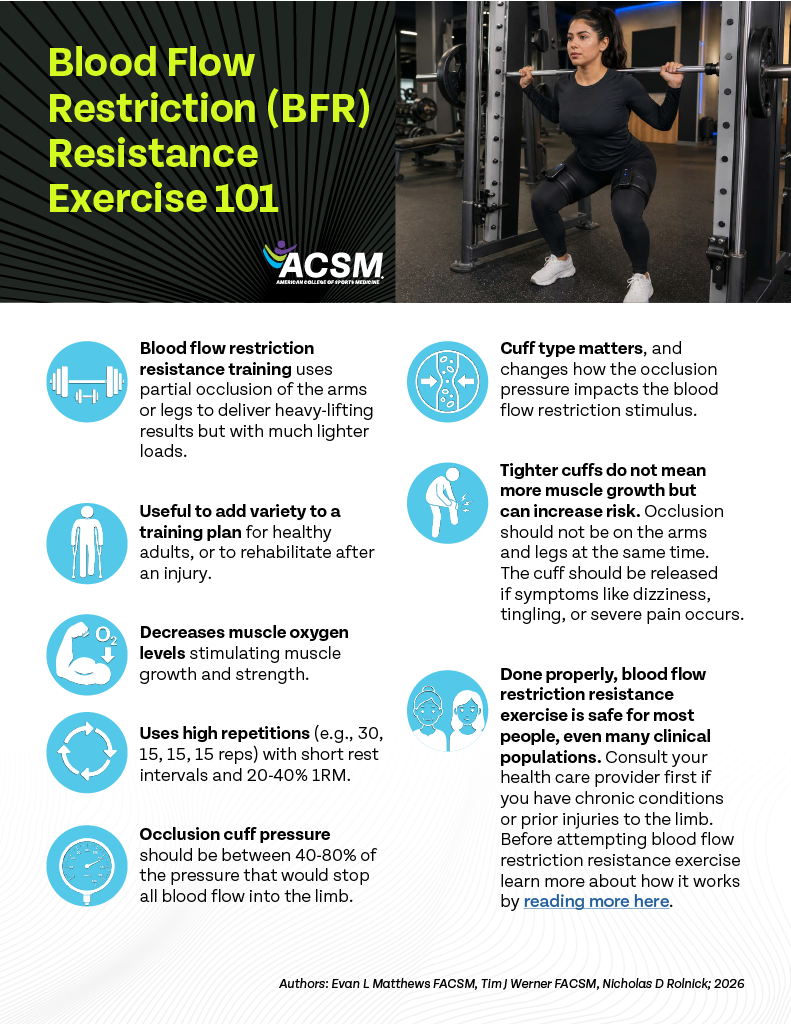
Blood flow restriction (BFR) resistance exercise is a method that uses a specialized cuff to partially limit blood flow during training. This approach allows for strength and muscle gains similar to heavy lifting, but with lighter weights and less joint stress. It is especially useful when high-load training is not practical or possible.
Click image to download PDF and read more below.
What is BFR Resistance Exercise?
BFR is using an inflated occlusion cuff, similar to a blood pressure cuff, wrapped around the upper legs or arms to reduce blood flow in and out of the limb during exercise. The cuff pressure is usually high enough to stop blood from leaving the limb (venous blood flow), but not high enough to fully stop blood from entering the limb (arterial blood flow). It can be done during resistance or aerobic exercise or even applied at rest, but the focus of this document is on BFR resistance exercise.
Why do BFR?
BFR resistance exercise leads to strength improvement and muscle growth comparable to traditional strength training, but with lower impact on the joints. The lower joint stress is because BFR resistance exercise usually involves lifting much lighter weights than typically used in strength training. It can be useful to add variety to a training plan for healthy adults, but the best-case use is when heavy weights are not possible (e.g., injury, frailty, certain clinical populations).
How Do You Do BFR Resistance Exercise?
BFR resistance exercise typically uses high repetitions, low weight, and low rest durations more similar to training for local muscular endurance, but while having the occlusion cuff inflated on the exercising limb. The lower muscle blood flow reduces muscle oxygen levels comparable to heavy weight training (Perlet et al., 2024). The most common programs include 4 sets of 30, 15, 15, 15, 15 repetitions (similar benefits are seen with all sets of 15 (de Queiros et al., 2024)) or 4 sets to failure using 20-40% of one-repetition maximum and
30-60s of rest between sets. The cuff pressure can be maintained or deflated during the rest period depending on client’s tolerance (Patterson, 2019).
Ideally, the occlusion cuff should be inflated to between 40-80% of the pressure that would stop all blood flow into the limb (i.e., arterial occlusion pressure (AOP)). The cuff type, width, material, placement, etc. affects the pressure needed to fully stop blood flow (Rolnick et al., 2023). Therefore, the AOP should be assessed with the same cuff used during the BFR exercise. Automated systems exist for assessing AOP and performing BFR exercise making these systems highly user friendly. Multi-chamber cuffs also exist that prevent full occlusion even at high pressures (Rolnick et al., 2023). Using multi-chamber cuffs, prior research has inflated to pressures of 250 mmHg for the upper body and 350 mmHg for the lower body (Early et al., 2020). While sub-optimal and imprecise, non-inflatable occlusion bands/straps also exist and is typically tightened to a 6 out of 10 level (Aniceto & da Silva Leandro, 2022; Bielitzki et al., 2021). Regardless of cuff type used, restriction should typically last less than 10 continuous minutes, a pulse should be palpable in the limb below the cuff, and cuffs should be released if numbness or tingling occurs. It is important that exercisers do not adopt a tighter is better approach to the restriction as this does not improve strength benefits and can lead to unnecessary risk.
Who Should Avoid BFR Resistance Exercise?
The primary safety concerns with BFR resistance exercise are blood clots, increased cardiac stress vs other forms of resistance exercise, (Patterson et al., 2019) and excessive muscle damage (Rolnick et al., 2021). The available literature does not suggest an increased risk of blood clots with the use of BFR, even in at risk populations, but this research is ongoing. BFR resistance exercise does increase cardiac stress by increasing the heart rate and blood pressure while decreasing the stroke volume compared to exercise without BFR. These effects can be minimized by releasing the cuff during each rest interval. While BFR resistance exercise has been safely used in cardiac populations (Angelopoulos et al., 2023; Cahalin et al., 2022), it may be wise to consult your health care provider before engaging in BFR resistance exercise if you are at high risk for blood clots or cardiac stress related adverse events (Nascimento et al., 2022). The risk of excessive muscle damage leading to negative health outcomes (e.g., rhabdomyolysis) is likely similar for BFR resistance exercise compared to traditional strength-oriented resistance exercise despite the lower loads used (Wernbom et al., 2021). Therefore, excessive loads, high repetition volumes, long restriction times, and training to failure should be avoided in the initial weeks of BFR resistance training.
The reference for all this information unless another citation is given is: (Patterson et al., 2019)
Reference list
Aniceto, R. R., & da Silva Leandro, L. (2022). Practical Blood Flow Restriction Training: New Methodological Directions for Practice and Research. Sports Medicine – Open, 8(1), 87. https://doi.org/10.1186/s40798-022-00475-2
Bielitzki, R., Behrendt, T., Behrens, M., & Schega, L. (2021). Current Techniques Used for Practical Blood Flow Restriction Training: A Systematic Review. Journal of Strength & Conditioning Research, 35(10), 2936–2951. https://doi.org/10.1519/JSC.0000000000004104
de Queiros, V. S., Rolnick, N., Schoenfeld, B. J., Martins de França, I., Vieira, J. G., Sardeli, A. V., Kamis, O., Neto, G. R., Cabral, B. G. de A. T., & Dantas, P. M. S. (2024). Hypertrophic effects of low-load blood flow restriction training with different repetition schemes: a systematic review and meta-analysis. PeerJ, 12, e17195. https://doi.org/10.7717/peerj.17195
Early, K. S., Rockhill, M., Bryan, A., Tyo, B., Buuck, D., & McGinty, J. (2020). EFFECT OF BLOOD FLOW RESTRICTION TRAINING ON MUSCULAR PERFORMANCE, PAIN AND VASCULAR FUNCTION. International Journal of Sports Physical Therapy, 15(6), 892–900. https://doi.org/10.26603/ijspt20200892
Nascimento, D. da C., Rolnick, N., Neto, I. V. de S., Severin, R., & Beal, F. L. R. (2022). A Useful Blood Flow Restriction Training Risk Stratification for Exercise and Rehabilitation. Frontiers in Physiology, 13, 808622. https://doi.org/10.3389/fphys.2022.808622
Patterson, S. D., Hughes, L., Warmington, S., Burr, J., Scott, B. R., Owens, J., Abe, T., Nielsen, J. L., Libardi, C. A., Laurentino, G., Neto, G. R., Brandner, C., Martin-Hernandez, J., & Loenneke, J. (2019). Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Frontiers in Physiology, 10. https://doi.org/10.3389/fphys.2019.00533
Perlet, M. R., Hosick, P. A., Licameli, N., & Matthews, E. L. (2024). Microvascular Reactivity Is Greater Following Blood Flow Restriction Resistance Exercise Compared with Traditional Resistance Exercise. Journal of Strength and Conditioning Research, 38(10), e553–e562. https://doi.org/10.1519/JSC.0000000000004873
Rolnick, N., Kimbrell, K., Cerqueira, M. S., Weatherford, B., & Brandner, C. (2021). Perceived Barriers to Blood Flow Restriction Training. Frontiers in Rehabilitation Sciences, 2, 697082. https://doi.org/10.3389/fresc.2021.697082
Rolnick, N., Kimbrell, K., & de Queiros, V. (2023). Beneath the cuff: Often overlooked and under-reported blood flow restriction device features and their potential impact on practice—A review of the current state of the research. Frontiers in Physiology, 14. https://doi.org/10.3389/fphys.2023.1089065
Wernbom, M., Paulsen, G., Bjørnsen, T., Cumming, K., & Raastad, T. (2021). Risk of Muscle Damage With Blood Flow-Restricted Exercise Should Not Be Overlooked. Clinical Journal of Sport Medicine : Official Journal of the Canadian Academy of Sport Medicine, 31(3), 223–224. https://doi.org/10.1097/JSM.0000000000000755